

Case: Ben
Identifying data |
|
Reason for Referral |
|
Chief complaint / Goals |
|
History |
|
What are you going to recommend to support Ben?
Quiz
Which of the following is FALSE?
- The majority of people who experience a traumatic event will develop PTSD.
- Severity, frequency and duration of an adverse event increase the risk for PTSD.
- Mindfulness practice reduces the risk for PTSD.
- Children who have experienced developmental trauma frequently are given multiple psychiatric diagnoses.
- PTSD can be diagnosed at any age.
A patient with PTSD has not responded to an initial trial of classic cognitive behavior therapy (CBT). Which is TRUE?
- The patient clearly has poor motivation. Ask the patient to return when they are motivated to seek treatment.
- One should start a course of SSRI.
- One should start a course of antipsychotics.
- If classic CBT that targets the “rational brain” hasn’t worked, it may mean that lower level interventions targeting the “emotional” or “survival brain” are required, such as help with self-regulation first, or subcortical therapies (e.g. EMDR).
- One should try another course of classic CBT, with a different therapist.
Introduction
On one hand, stresses are a part of human existence. In fact, human beings require sufficient amounts of “healthy stress” in order to grow and develop. Life without any stress at all is boring and unfulfilling.
Stresses include day-to-day stresses at home, school and work.
On the other hand, when stresses become excessive, then it becomes "toxic" stress.
How Common is Trauma and Adverse Childhood Experiences (ACEs)?
Studies show that it is very common to experience ‘adverse experiences in childhood’ (ACEs).
Adverse childhood events include (Felitti, 1998):
- Physical (30%)
- Emotional abuse (11%),
- Sexual abuse (19%)
- Emotional or physical neglect
- Family member with alcohol abuse (25%) or drug abuse (5%);
- An incarcerated household member
- A family member with mental illness (19%)
- Witnessing their mothers being treated violently (12.5%)
- One or no parents
Unfortunately:
- Most people (2/3) have had at least one adverse childhood event (ACE) in their lives;
- One in five had > 3 ACEs
- Persons who have experienced >3 ACEs have
- 4-12X increased health risks for alcoholism, drug abuse, depression, and suicide attempt
- 2-4X increase in smoking, poor self-rated health, ≥50 sexual intercourse partners, and sexually transmitted disease
- 1.4-1.6X increase in physical inactivity and severe obesity.
Epidemiology
Most people (2/3) have had at least one adverse childhood event in their life.
Many people (15-43%) have had at least one trauma
- 15-43% of girls will experience trauma → 3-15% will go on to develop PTSD
- 14-43% of boys will experience trauma → 1-6% will; go on to develop PTSD
Prevalence of PTSD in children/adolescents
- 4 – 6 %
In summary:
- Adverse childhood events and traumas are common; fortunately, most of the time, people do not go onto develop clinical PTSD.
Risk Factors (including Predisposing, Precipitating and Perpetuating) for PTSD
Why do some people develop PTSD?
Predisposing factors may include:
- Sensitive temperament
- Pre-existing psychiatric illness
- Family history
Precipitating may include:
- Trauma that is more severe, more frequent, or longer in duration
- Trauma that led to a sense of helplessness or loss of control
- Prolonged or repeated exposure.
- Poor social support system.
- Recent life stressors or changes
Perpetuating
- Once PTSD has occurred, symptoms of PTSD may further disconnect the person from activities / people that bring purpose, hope, belonging and meaning.;
- Unhealthy coping strategies such as turning to alcohol/substances, excessive screen time or other potentially addictive strategies.
What Types of Trauma Are Most Associated with PTSD?
The most common traumas leading to PTSD are:
- Disasters – natural or man-made
- Violent crimes – kidnapping, rape, murder of a parent, school shootings
- Motor vehicle accidents
- Severe burns
- Exposure to community violence
- War
- Peer suicide
- Physical or sexual abuse
Neuropathophysiology of Trauma
Brain basics (Van der Kolk 2014)
- The brain is organized in a lower-to-higher manner from both evolutionary and developmental perspectives
- Lowest and oldest – the reptilian brain: brainstem and hypothalamus, in charge of “housekeeping” basics like breathing, heart rate, temperature control
- Next – the mammalian, or limbic brain: in charge of monitoring for danger, emotions and emotional relevance of input, contextualizing
- Highest and newest – the neocortex: planning, reflection, language, abstract thought, judgment and implementation, sense of time and context, empathy
- Healthy neurobiology means good connectivity between these areas and that they function properly; i.e. a state of integration exists
Normal threat response
- Multiple sensory inputs converge in the thalamus (= the cook) where they are integrated into a coherent pattern (the stew) and sorted for relay onward
- The sensations are then relayed both down to the amygdala and up to the frontal cortex (a slower relay)
- Amygdala = the smoke detector
- Perceived threat -> amygdala sends message to hypothalamus and brainstem -> stress hormones and autonomic nervous system (ANS) respond -> whole body is prepared for defense
- The medial prefrontal cortex (MPFC) is the watchtower which allows us to stop-think-respond
Trauma alters brain systems
- When a stress or trauma is severe enough, it overwhelms the brain’s ability to cope and process.
- The Alarm System (“Fight, flight, freeze”) activates.
- Amygdala becomes overactive, hyperalert for possible danger, stress hormones are chronically increased
- The Filter: Thalamus’ ability to integrate sensory inputs compromised; events may be recorded as an incoherent jumble of sights, sounds, etc.
- Memory System: Cortisol blocks hippocampal function which blocks memory formation; memories may be non-coherent, non-verbal and non-narrative
- Stop-and-think system: Activity of the medial prefrontal cortex (MPFC) is reduced when intense fear, anger, and sadness increase the activation of subcortical brain regions, leading to failure of emotion regulation, loss of reflective ability, impulsive reactivity.
Trauma causes different symptoms at different levels of the brain:
| Following trauma, people try to process and make meaning of the trauma, which explains cognitions such as:
|
| |
| Visual images – pictures of the memory may intrude |
| Emotional dysregulation, such as unprocessed anger, fear, hurt, sadness, guilt, shame. |
| The body has its own memory, which can lead to somatic flashbacks, whereby the person relives the physical sensations that happened during the traumatic experiences. |
| Body’s alarm system becomes chronically activated, leading to hypervigilance, easily startled, “fight/flight/freeze” response. Chronic fight/flight/freeze can lead to “shut down” such as dissociation. |
Clinical Presentation
After a trauma, people may experience all manner of symptoms including:
- Emotional
- Avoidance of thoughts, feelings and conversations associated with the trauma 83%
- Distressing recollections 70%
- Inability to recall important aspects of the trauma 70%
- Disturbing dreams 64%
- Difficulty concentrating 64%
- Emotional lability
- Mood symptoms such as anxiety, depression
- Attachment and interpersonal problems
- Cognitive
- Alterations in cognitive function
- Re-experiencing – nightmares, intrusive memories, flashbacks, traumatic repetitive play
- Avoidance of memories or situations that are reminders
- Behaviour
- Unpredictable/impulsive behaviour
- Behavioural inhibition or activation
- Aggression due to “fight” being activated
- Avoidant behaviours when “flight” has been activated
- WIthdrawal when “freeze” or shutdown.
- Regression, e.g. child acts like a younger child, e.g. needing to sleep in parent’s bed; losing bladder control.
- Revictimization, i.e. tendency to continue to end up in unsafe situations.
- Behavioural reenactment
- Children may act out the trauma, as through repetitive play
- E.g. a young child playing with dolls may recreate scenes of trauma
- With sexual abuse
- Sexual promiscuity, inappropriate sexual behaviours
- Difficulties with physical contact (for abuse)
- Autonomic and self-regulation
- Increased arousal and hypervigilance
- Problems with self-regulation
- Intense reactions to triggers
- Medical / physical
- Somatic complaints such as headaches, stomach aches, muscle aches, etc.
- Sensory sensitivities, such as over or under-reaction to noise, physical contact, lightning, sudden movement
- Other
- Sleep problems
- Flashbacks:
- Not common in young children
- Functional impairment
- Inconsistent academics
- Addictions
- May turn to addictive behaviours, such as alcohol, substance use or screen addictions (when old enough to have access).
Triggers
- Being exposed to situations or reminder of trauma can trigger symptoms, e.g. anniversary reminders; seeing a past abuser; having been exposed to sexual abuse and then being triggered when seeing a film about sexual abuse.
Effects of Trauma by Age
The younger the age that trauma occurs at, the more it will interrupt normal development, and thus the more impairment it will cause.
Age 0-5 (Infants, toddlers, preschoolers) |
|
With children/youth |
|
Delayed effects
- Trauma can occur at a younger age, though problems may not seem to be apparent until later.
- For example
- Child abuse between ages 4-8 tend not to have depression until puberty - “silent period”; high onset of depression after entering puberty
- Youth with an ACE score of 5 or more show a large increase in drug and binge drinking after age 20 – delayed onset
Intergenerational trauma
- As a traumatized child becomes an adult, there is a risk of intergenerational trauma. Negative self-perceptions arising from disordered attachment set people up for further abuse and negative experiences.
- For example
- If a person lacks an internal sense of security it is difficult to distinguish between safety and danger.
- If you feel chronically numb, you may choose dangerous or risky situations as they make you feel “alive” (as opposed to avoiding them).
- If you know you are a terrible and worthless person, you may choose negative situations that repeat what you have become accustomed to;
- Feelings become facts, e.g. the person feels worthless, they think they must be worthless.
Assessment of Trauma
Remember that even talking about trauma can be re-traumatizing. You might say something such as:
- “I’d like to ask you about stressful past experiences in your life. But if it’s too stressful to talk about it, feel free to let me know. Will you be able to let me know?”
- “What have been the most stressful, scary, traumatic events in your life?”
- Try to get a brief list, without getting too much detail
- “On a scale between 0 and 10, where 10 is the most stressful, how stressful was it?”
- “How have these experiences affected you?”
Specifics symptoms
- “Since the trauma(s), have you had any problems such as...
- “Flashbacks, which is seeing / hearing / experiencing the past, like a movie being replayed?”
- “Problems at home? With school? Peers/relationships?
- “Avoidance of situations that remind you of the trauma?”
Diagnosis
DSM-5 Criteria for PTSD
For age 7 and up
- Exposed to death, threatened death, actual or threatened serious injury, or actual or threatened sexual violence
- Direct exposure; witnessing; indirectly (close relative or friend); repeated or extreme indirect exposure (as in work-related)
- Intrusion symptoms
- Avoidance
- Negative alterations in cognitions and mood
- Alterations in arousal and reactivity
- Duration > 1 month
- Distress or impairment
- Not attributable to another cause
Specifiers:
- With dissociative symptoms
- With delayed expression (full dx not met until at least 6 months after event)
For aged 6 and younger
- Exposed to death, threatened death, actual or threatened serious injury, or actual or threatened sexual violence
- Direct exposure; witnessing; indirectly (close relative or friend); repeated or extreme indirect exposure (as in work-related)
- Intrusion symptoms -- NOT REQUIRED
- Avoidance -- NOT REQUIRED
- Negative alterations in cognitions and mood -- NOT REQUIRED
- Alterations in arousal and reactivity
- Duration > 1 month
- Distress or impairment
- Not attributable to another cause
Developmental Trauma Disorder (DTD)
Unfortunately, there are shortcomings with DSM definitions and conceptualization of trauma such as:
- DSM-5 does not differentiate between
- Single episode events (e.g. accident)
- Cumulative events (e.g. experiencing war)
- Developmental trauma (e.g. prolonged and repeated and occurring during early development)
- DSM-5 does not adequately describe “little t” trauma such as chronic abuse, humiliation or bullying (though it does adequately describe “big T” trauma.
- DSM does not take into account developmental aspects of PTSD, that PTSD is a developmental disorder and an attachment disorder
- Heterogeneity of response - presentation can look different at different ages.
- Comorbid diagnoses common – are they really separate problems?
- *Children who fulfill 2 clusters of PTSD symptoms are as functionally impaired as those who fulfill 3 clusters (Carrion et al 2011).
Types of Trauma
Big “T” trauma such as
- A child who is exposed to overt abuse, such as physical, sexual abuse or neglect.
Little “t” trauma
- Parents may have been well intentioned, but perhaps there is a “poor fit”, e.g. a sensitive child with high emotional needs, however parents (for whatever reason) are unable to meet the child’s needs.
- What’s different with chronic early abuse?
- Less obviously trauma-related symptoms & behaviours
- Disruptive behaviours
- Poor frustration tolerance
- Depression/withdrawal
- Apathy/loss of interest in goals
- Anxiety/worry
- Poor concentration or focus
- Fighting
- Truancy
- Substance abuse
Differential Diagnosis (DDx): Psychiatric
After trauma, there are many possible sequelae, including medical and psychiatric, of which PTSD is one of them. Many other conditions can also present with symptoms that overlap with PTSD, such as mood, anxiety, autonomic arousal, cognitive symptoms, etc.
Psychiatric DDx (and comorbidity) includes:
Numerous conditions are more likely after trauma, including the following:
Condition | Questions |
Adjustment disorder | Any big stresses lately? Any troubles coping or adjusting to the stress? |
Major depressive disorder
| Any problems with depressed mood? |
Bipolar disorder
| Any episodic periods of increased activation (e.g. increased energy, irritability), that coincide with circadian rhythm disturbance (i.e. decreased need for sleep)? |
Anxiety disorders such as generalized anxiety, panic disorder, phobias, etc.
| Is your child a big worrier? What sorts of worries? |
Attention deficit hyperactivity disorder (ADHD)
| Prior to any trauma, were there troubles focusing or paying attention? Any hyperactivity, such as troubles sitting still, or constantly moving? |
Oppositional defiant disorder
| Any problems with oppositionality and defiance? |
Attachment problems (e.g. Reactive attachment disorder of childhood)
| Did the child have any troubles connecting or attaching to caregivers? Avoidant? Or clingy? |
Substance and alcohol use
| Any use of substances / alcohol that cause problems?
|
Psychosis | Hearing things that others do not? Seeing things that others do not? Are there any people out to harm you? |
Delirium | Any fluctuating level of consciousness? Disturbed sensorium? |
Differential Diagnosis (DDx): Medical
There are various medical conditions that can contribute to autonomic or other symptoms that resemble or contribute to aspects of PTSD:
Condition | Questions |
General complaints
| Any problems with headaches? Stomach aches? Other aches/pains? |
Endocrine
| |
| Any complaints of being much hotter than others? Any complaints of being much colder than others |
Neurologic
| After the trauma, any problems with: * Migraines * Memory? * Concentration? * Headaches? * Fatigue? |
| Any seizures/convulsions? Any times when parts of your body move without your control, e.g. twitching, jerking, shaking, going limp? Any spacing out? Any usual “spells”? |
Respiratory
| Any problems breathing? Any problems with coughing, wheezing? |
Sleep disorder | Problems with sleeping? Did these problems exist prior to the trauma? |
Cardiovascular
| Are symptoms worsened by being upright, along with fatigue that leads patient to sit or lie down? |
Medications
| Any use of caffeine or stimulants? |
Physical Exam
Vitals | Any signs of autonomic arousal such as:
|
General | Any visible signs of injury or trauma, e.g. head? Any signs of intoxication? (suggesting substance use issues) Any signs such as self-cutting, suggesting attempts to cope with emotional dysregulation? Any signs of “flight”, e.g. Easily started? Any signs of “fight”, e.g. aggressive, irritable? |
Investigations
There are no laboratory investigations for diagnosing PTSD currently. However, investigations may help with assessing for associated conditions:
Condition | |
Thyroid ● Hyperthyroidism can lead to restlessness, insomnia, autonomic hyperactivity, which are also seen in PTSD | Thyroid indices such as ● TSH ● Free T4 |
Neurologic ● If the trauma was physical (e.g. motor vehicle accident, physical assault), , there may be traumatic brain injuries such as concussion | Brain imaging |
● Sleep disorder | Sleep studies |
Substance use | Urine screening |
Management of Trauma: Trauma Informed Care
Trauma-Informed Care
Trauma-informed care is an approach where health providers recognize that patients are more likely to have been exposed to stressful, traumatic and adverse childhood events (ACE), than not. Acknowledging the role of trauma changes how we might approach and support a child, youth or parent.
1. Safety – need a secure base. Example:
- State conditions of treatment including
- Confidentiality
- Schedule,
- Patient’s right to choose to talk or not -- if your patient is not able to talk, validate that they may not feel safe or ready to talk, and that they can talk whenever they feel safe or ready.
- If they cannot talk, talk about less distressing topics, or help them with self-regulating strategies.
2. Structure
- Cognitive-affective-cognitive sandwich (structure – emotion>calming – structure) in every session; ensure that pt leaves in good shape
- Start with cognitive, e.g. “What happened?”
- Then proceed to emotional content, e.g. “How did you feel about that?” Or “How do you react?”
- Then go back to cognitive.
3. Success – One step at a time.
- With therapy, go one step at a time. Provide gratitude for successful steps.
- Personal trainer approach to build up a track record of success.
- Examples of success include:
- Clinician: “Despite all that you have been through, you have been able to come here today. Thank you so much for that.”
- Clinician: “Despite all that you have been through, you have still managed to look after your cat. Thank you so much for that.”
- Etc..
Management Principles: Neurosequential Treatment
Trauma results in a fundamental reorganization of the way mind and brain manage perceptions.
It changes multiple levels including:
- Cortical level: It changes how one thinks, what one thinks about, and one’s very capacity to think.
- Talking therapies tend to intervene at the cortical level, with helping victims of trauma find the words to describe what has happened to them is profoundly meaningful.
- However, if there is significant subcortical distress, then cortical interventions are not enough.
- Telling the story doesn’t necessarily alter the automatic physical and hormonal responses of bodies that remain hypervigilant, prepared to be assaulted, or violated, i.e. telling the story doesn’t necessarily change the subcortical.
- Subcortical interventions
- Subcortical interventions help the body learn that the danger has passed and that one can live in the reality of the present (as opposed to being stuck in the past).
- The problem is not only cortical, but also subcortical.
Two Strategies for Improving Self-Regulation
Self-regulation is impaired after trauma. One can teach self-regulation (including emotional regulation) in two ways:
- Top-down regulation:
- Engage the thinking brain (psychotherapy);
- Strengthen the capacity of the MPFC (e.g. mindfulness).
- Bottom-up regulation:
- Learning to recalibrate and manage the autonomic nervous system
- Enhancing parasympathetic regulation, targeting subcortical systems
- Eg breathwork, yoga, body work, vagal tone enhancement.
- “Story follows state”, i.e. if one can help the person’s “state” (i.e. autonomic nervous system, subcortical system), then it will help them with their thoughts and feelings (i.e. their “story”).
Evidence-Informed Trauma Therapies
Trauma-specific therapies
- EMDR - good evidence
- EMDR – Level 1 evidence with adults – focus on the worst moment(s) during eye movements
- Good evidence for efficacy of EMDR with children
- May be more effective than CBT
- May provide relief in shorter time
- Can be very effective for single episode trauma
- Requires training and specific procedure
- Trauma-focused CBT - good evidence
- TF-CBT – write/draw the story page by page, parent involvement and coaching. The best studied
- Empirical evidence: 9 RCTs compared to usual care or active comparison conditions like play therapy, client centered therapy cognitive therapy
- TFCBT superior to ‘other’ treatments in improving PTSD, depression, anxiety, fear, externalizing behaviour problems, shame – few comparisons to brain-based treatments which show promise
- Also superior to other treatments in improving parental outcomes
- Other CBT treatments likely similar outcomes
- Prolonged exposure therapy
- Involves the client telling your story over and over.
- Unfortunately, difficult to do in the real world as this is difficult to tolerate for clients and has a high dropout rate.
Psychodynamic psychotherapy
- Emotion regulation therapies
- Dialectical behavior therapy
- Mentalization-based therapy
- Acceptance and Commitment Therapy (ACT)
Promising practices
- These are practices which have growing evidence, though not yet sufficient evidence to be recommended in clinical practice guidelines such as
- Brainspotting
- Directly accessing subcortical brain via visual points “where we look affects what we feel”
- Allows very rapid processing for either painful memories or less acutely distress things/anxieties
- “Where we look affects how we feel” – uses focus spots in the visual field to access neural networks and process emotional material and memories
- Can be used with specific or nonspecific trauma memories
- Can also be used for processing worries, anxieties, etc
- Client does not have to talk about “it” – that’s optional
- Evidence – very early; interesting comparison of treatments post Sandy Hook shooting indicated that BSP was more effective than EMDR, TFCBT, supportive
- Progressive counting
- Easy to learn to use, efficient, effective, well tolerated; multiple imaginal exposures per session, increasingly longer till SUDs go down
- Early evidence indicates that Progressive Counting may be as effective as EMDR but easier for pt (and therapist), and faster
- Probably a combination of subcortical-cortical work
- Client does imaginal exposure by running through a mental movie of the target memory in controlled, progressive longer, time (10 sec -> 100 sec)
- Therapist tracks the distress level
Parenting Skills
Healthy attachment
Teaching validation skills, empathy, self-compassion
- Teaching active positive response
- Attachment education: children require secure attachments to thrive
- How to improve attachment relationships with your child(ren)
Psychoeducation about Stress and Trauma
- Teach child about how body reacts to stress
- Teaching focused breathing
- Even belly breathing, with or without counting
- Can teach 1:2 breathing
- Mindfulness breathing and meditation techniques
- Progressive muscle relaxation
- Therapist or parent can make a recording of themselves so that patients have the recording for future reference.
- Parents need relaxation and self-care too
- Resources
- MindMasters for children
- Calm.com for youth
- Mindshift
Psychoeducation about Emotional Regulation
- Work on identifying and naming feelings
- Provide parent with sessions to talk about their own feelings
- Help parents encourage children to express emotions verbally and to listen
- Thought interruption: channel changing
- Positive imagery – safe place
- Positive self-talk
Teaching Resilience to Clients and Families
Some resilience is inherent (temperament), however most resilience can be taught and learned. After a trauma, there is the potential to grow and become stronger from the trauma.
Help your patients and families to:
- Positive relationships: cultivate secure attachments
- Positive emotion: cultivate positive experiences
- Social interactions
- Fun
- Relaxation
- Self-care
- Conscious recognition of positives: eg WWW+W (What Went Well and Why)
- Cultivate people and activities that give a sense of meaning, belonging and purpose (i.e. accomplishment) (Seligman, 2011).
Phase Model of Treatment
Regardless of the specific type of trauma treatment, therapy works in various stages. The therapist does not start by exploring and talking about the trauma in depth. Rather, there are various steps and stages such as:
History
- Do a trauma / loss history
- Thoughts/meaning: What would someone learn from this (trauma/loss) experience?
- Feelings: What kinds of feelings might be piled up?
- What are the problematic behaviours?
- What are person’s triggers?
- I.e. what are the situations, or thoughts that trigger distress?
Psychoeducation
- Education, validation, formulation and meaning
- Talking with the person about how their reactions make sense, given their experience.
- Clinician: “It would make sense that you feel anxious around ___, because of the experiences you have had.”
Enhance safety
- Ensure that home, work and relationships are safe
- Avoid danger situations
Support self-regulation
- Consider using self-regulation plans / safety plans
Does the client need and/or want to process certain memories?
- If so, then do specific traumatic subcortical memory processing interventions, depending on the therapeutic intervention being used, such as EMDR, brainspotting, progressive counting, etc.
Medications for PTSD and Trauma in Children/Youth
Have non-medication options been tried without success? Consider medications for specific symptoms.
Unlike adults, there is much less evidence to guide treatment in children/youth. There are no trials supporting any specific medications for PTSD per se.
Is there PTSD, without anxiety or depression? | If YES → | Current evidence does not support the use of SSRIs as first-line treatments for PTSD alone in children and adolescents (Strawn, 2010). No differences in PTSD symptom reduction were seen between SSRI compared with placebo in multiple small randomized trials with:
|
Is there anxiety or depression? | If YES → | SSRIs
|
Is there autonomic hyperarousal, intrusive nightmares? | If YES → | Antiadrenergic agents
|
Are there nightmares? | If YES → | Cyproheptadine (Periactin)
|
Are there still difficulties? | If YES → | Some evidence suggests the following might be helpful, though unfortunately, no RCTs are available (Keeshin et al., 2014)
|
Is there PTSD plus comorbid depression anxiety?
- Although evidence for PTSD alone appears negative, consider SSRIs if there is comorbid depression/anxiety
Medications for PTSD / Trauma in Adults
The Veteran’s Administration (VA) makes various recommendations for medications for PTSD in Adults:
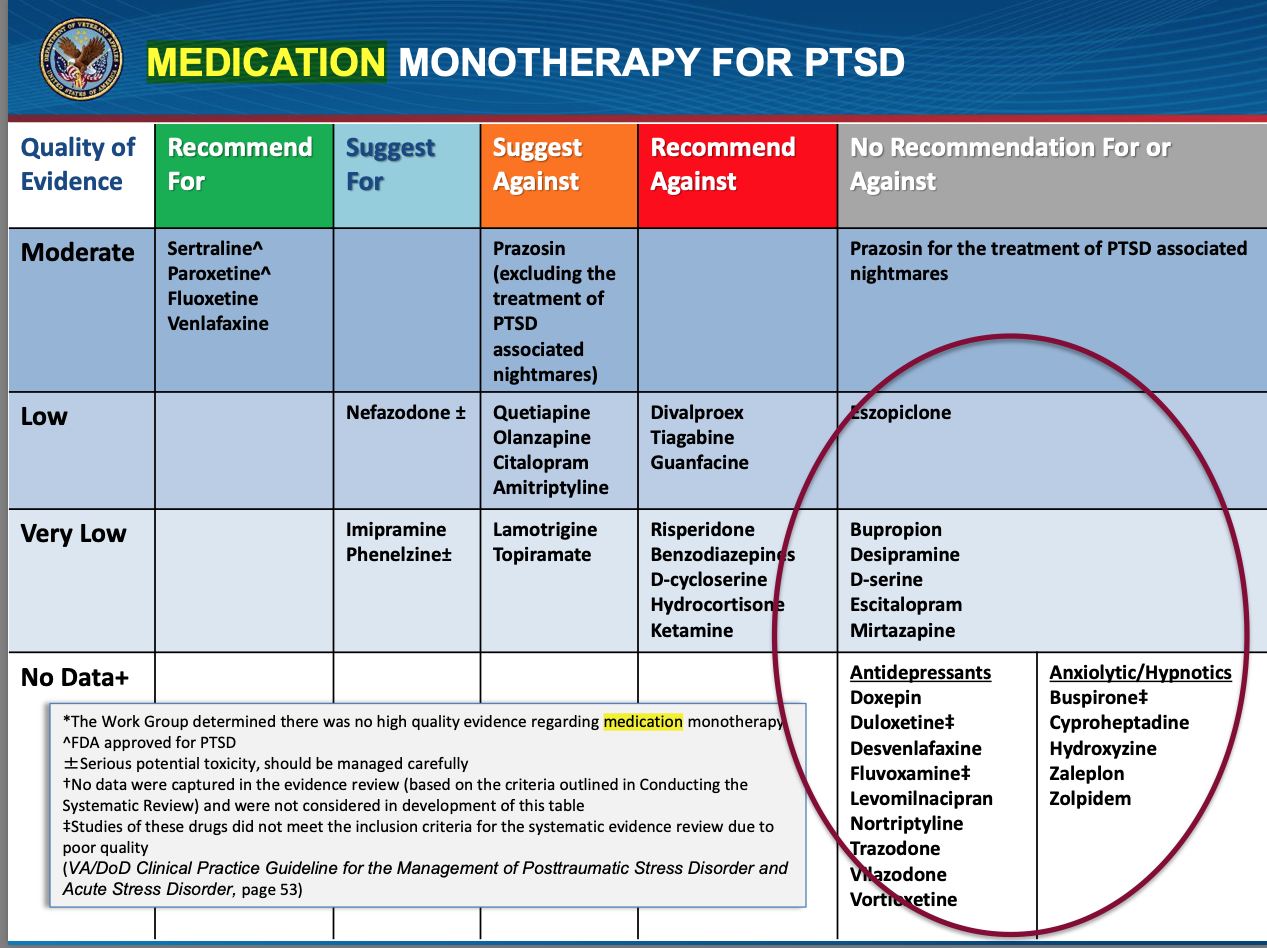
Examples
- SSRIS
- Sertraline (FDA approved for PTSD)
- Paroxetine (FDA approved for PTSD)
- Fluoxetine
- SNRI
- Venlafaxine
- Atypical antidepressants used for sedative properties
- Mirtazapine,
- Trazodone,
- Nefazodone
- α-Adrenoreceptor antagonists.
- Prazosin
- Atypical antipsychotics, though not
- Risperidone
- Quetiapine
On the other hand, the Veteran’s Administration (VA) recommends against the following as monotherapy
- Quetiapine,
- Olanzapine,
- Generation Antipsychotics (except for Risperidone, which is a Strong Against)
- Citalopram
- Amitriptyline
- Lamotrigine
- Topiramate
- Divalproex
- Tiagabine
- Guanfacine
- Risperidone
- Benzodiazepines
- Ketamine
- Hydrocortisone • D-Cycloserine
The VA also recommends against cannabis, on the basis of population level side effects (e.g. increased risk of psychosis) and lack of RCTs for cannabis.
Prevention of PTSD
Is it the first 3-months after trauma exposure?
- Provide information, emotional support, practical assistance (as opposed to individual psychological debriefing) (Australian Guidelines for Prevention and Treatment of Acute Stress DIsorder, PTSD and Complex PTSD, 2020)
https://app.magicapp.org/#/guideline/Edr04L
Specific Strategies
Enhance protective factors after the trauma | Ensure that there is family and other supports that the person can turn to.
|
Help the patient make positive meaning from the experience | Clinician: “The fact that this trauma happened, what do you think this means?” If the patient has a negative attribution, e.g. this happened to me because I’m a bad person”, try to come up with a more positive, self-compassionate attribution such as : “Bad things happen, even to good people; its part of being human; there is nothing wrong with me; its okay to feel sad, I will get through this…” |
Basic psychoeducation | Elements of basic psychoeducation include:
|
Medications
Are there medications that can be given shortly after a trauma to prevent post-traumatic stress symptoms?
- A few studies have looked at using medications (mainly in adults) following acute trauma, though there is not much data.
- Most have focused on medications which decrease memory consolidation and decrease physical arousal
- Propranolol
- Prazosin
- Morphine (burn victims) – Pain control is important!
- Imipramine
- Some studies involve strategies such as playing Tetris shortly after trauma may be helpful. By “flooding” the visual cortex with visual stimuli from the video game, it helps block out visual memories of the trauma.
Insufficient evidence to suggest medications for prevention of trauma.
Management of Trauma: Self-Care for Health Providers
Self-care is important, as working with victims of trauma can lead to stress, burnout and even PTSD symptoms, through “vicarious trauma”, which is defined as:
- “… the transformation that occurs within the therapist (or other trauma worker) as a result of empathic engagement with clients’ trauma experiences and their sequelae.” (Pearlman & MacIan, 1995)
- “…clinicians who work with sexually abused clients or other victims of trauma may experience profound psychological effects, effects that can be disruptive and painful for the helper and can persist for month and years...” (McCann & Pearlman, 1990a; Pearlman & Saakvitne, 1995))
It is good to be empathic, however, mental health workers need boundaries to protect themselves.
Do’s
- Acknowledge that the work will affect you
- Create and maintain a healthy balance to minimize the effects of vicarious traumatization
- Be attentive and mindful of your “unique warning signs” that you need a break, e.g. when you have trouble sleeping thinking about your patients; when you feel “no one understands me”, i.e. feel all alone; etc.
Case: Ben, Part 2
Identifying data | 11 year old boy living with his adoptive parents and his biological sister. |
Reason for Referral | You are asked to see Ben for oppositional defiant behaviours. |
Your diagnostic assessment shows:
- He does NOT have ADHD
- He does meet criteria for PTSD as he has had
- Trauma
- PTSD symptoms such as re-experiencing and hyper vigilance, which lead him to be easily triggered by many day-to-day situations.
Your recommend the following
- Trauma-informed approach such as
- Parents and school understand him from “What has happened to this child?” Versus “What is wrong with this child?”
- Not simply punishing behaviours, but trying to understand the triggers and help with self-regulation for example
- Appreciating that he is triggered by noise, and thus trying to reduce noise when possible as opposed to simply expect him to “deal with it”
- Using radical empathy, acceptance and validation for frustration and anger as opposed to simply expecting him to “calm down!”
- Using non-talking strategies such as soothing sensory strategies (e.g. jumping on trampoline, movement breaks, butterfly hugs, etc) as opposed to expecting him to be able to talk.
- Treatment approach that is neurosequential that
- Starts with ensuring sensory, motor and self-regulation needs addressed, e.g. making a self-regulation plan.
- Evidence-informed trauma therapy (e.g. trauma-focused CBT) with a therapist experienced in trauma, with a goal to eventually help him work through and process past traumatic experiences, but only after an initial phase of work on helping with self-regulation and safety planning.
Post-Quiz
Which of the following is FALSE?
- The majority of people who experience a traumatic event will develop PTSD (FALSE)
- Severity, frequency and duration of an adverse event increase the risk for PTSD (TRUE)
- Mindfulness practice reduces the risk for PTSD (TRUE)
- Children who have experienced developmental trauma frequently are given multiple psychiatric diagnoses (TRUE)
- PTSD can be diagnosed at any age (TRUE)
A patient with PTSD has not responded to an initial trial of classic cognitive behavior therapy (CBT). Which is TRUE?
- The patient clearly has poor motivation. Ask the patient to return when they are motivated to seek treatment. (FALSE)
- One should start a course of SSRI. (FALSE)
- One should start a course of antipsychotics. (FALSE)
- If classic CBT that targets the “rational brain” hasn’t worked, it may mean that lower level interventions targeting the “emotional” or “survival brain” are required, such as help with self-regulation first, or subcortical therapies (e.g. EMDR). (TRUE)
- One should try another course of classic CBT, with a different therapist. (FALSE)
Clinical Practice Guidelines
All Ages
Australian Guidelines for the Prevention and Treatment of Acute Stress Disorder, Posttraumatic Stress Disorder and Complex PTSD
https://www.phoenixaustralia.org/australian-guidelines-for-ptsd/
Children /Youth
Cohen JA et al.: Practice Parameter for the Assessment and Treatment of Children and Adolescents With Posttraumatic Stress Disorder, Journal of the American Academy of Child & Adolescent Psychiatry, Volume 49, Issue 4, 2010, 414-430,
https://doi.org/10.1016/j.jaac.2009.12.020 .
Adults
Practice Parameters for the American Psychological Association (APA) Clinical Practice Guideline for the Treatment of PTSD
https://www.apa.org/ptsd-guideline/ptsd.pdf
Australian Guidelines for the Prevention and Treatment of Acute Stress Disorder, Posttraumatic Stress Disorder and Complex PTSD.
https://www.phoenixaustralia.org/australian-guidelines-for-ptsd/
References
Felitti VJ, Anda RF, Nordenberg D, et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The Adverse Childhood Experiences (ACE) Study. Am J Prev Med. 1998;14(4):245-258.
Greenwald, Ricky. Child Trauma Handbook, Haworth, 2005
Grand, D. Brainspotting. 2006.
Herman, J. Trauma and Recovery. Basic Books 1997.
Hoskins M, Pearce J, Bethell A, et al. Pharmacotherapy for post-traumatic stress disorder: systematic review and meta-analysis. Br J Psychiatry. 2015;206(2):93–100. https://pubmed.ncbi.nlm.nih.gov/25644881/
Keeshin B, Strawn J: Psychological and Pharmacologic Treatment of Youth with Posttraumatic Stress Disorder: An Evidence-based Review, Child Adolesc Psychiatric Clin N Am, 2014 Apr, 23(2), 399–411.
http://dx.doi.org/10.1016/j.chc.2013.12.002
Keeshin BR, Strawn JR. Risperidone treatment of an adolescent with severe posttraumatic stress disorder. Ann Pharmacother 2009;43(7):1374.
https://journals.sagepub.com/doi/abs/10.1345/aph.1M219
Perry, B. The Boy Who was Raised as a Dog. Basic Books 2007.
Seligman M, Flourish, 2011.
Strawn JR, Keeshin BR, DelBello MP, Geracioti TD Jr, Putnam FW. Psychopharmacologic treatment of posttraumatic stress disorder in children and adolescents: a review. J Clin Psychiatry. 2010 Jul;71(7):932-41. doi: 10.4088/JCP.09r05446blu. Epub 2010 Apr 20. PMID: 20441729.
https://pubmed.ncbi.nlm.nih.gov/20441729/
Van der Kolk, Bessel. The Body Keeps the Score, Viking, 2004.
Canadian Organizations
For Professionals
Disaster Psychiatry Canada
Psychiatrists and mental health providers with an interest in disaster psychiatry.
https://dpc2018.wordpress.com/
For General Public
PTSD Association of Canada
Non-profit organization dedicated to helping those with PTSD.
http://www.ptsdassociation.com/
About This Document
Written by the mental health professionals at CHEO. Adapted from “PTSD in Children and Adolescents: Seminar for Psychiatry Residents”, delivered by Dr. Marjorie Robb, Staff Psychiatrist.
Disclaimer
This information is offered ‘as is' and is meant only to provide general information that supplements, but does not replace the information from your qualified expert or health provider. Always contact a qualified expert or health professional for further information in your specific situation or circumstance.
Creative Commons License
You are free to copy and distribute this material in its entirety as long as 1) this material is not used in any way that suggests we endorse you or your use of the material, 2) this material is not used for commercial purposes (non-commercial), 3) this material is not altered in any way (no derivative works). View full license at https://creativecommons.org/licenses/by-nc-nd/4.0/
 Printing This For Someone?
Printing This For Someone?




